Rescue tecniques
"How do you absorb all these impressions, provided by many different emergencies?" many friends wannted to know. Generally spoken, this was rarely a problem. Of course, their were some missions which we difficult to forget (a considerable amount of which are collected here) and even a few which should better be forgotten (reference avoided on purpose), but in most cases, it was a kind of pleasure being in a position to help under conditions where others were not. And "help" was not just a matter of rescuing lives and reducing morbidity, it was connected to the treatment of pain and suffocation. "How do you absorb all these impressions, provided by many different emergencies?" many friends wannted to know. Generally spoken, this was rarely a problem. Of course, their were some missions which we difficult to forget (a considerable amount of which are collected here) and even a few which should better be forgotten (reference avoided on purpose), but in most cases, it was a kind of pleasure being in a position to help under conditions where others were not. And "help" was not just a matter of rescuing lives and reducing morbidity, it was connected to the treatment of pain and suffocation. Whether or not this treatment was life-saving, that was almost of secondary value.
I have mentioned previously that intubation (introduction of a tube to the airways) have a central importance during the most serious missions – those which justifies the presence of a physician; – that I have developed a particular technique for it; and that I prefer the route through the nose, even in cases where this appears contraindicated. Most physicians prefer to bring the tube in through the mouth, which is badly tolerated (swallowing reflex) and therefore calls for ample supply of sedatives. Moreover, the nasal route enables intubation with ventilation postponed, as mentioned in some of these cases. I have utilized these principles on a rather broad indication, e.g. to confined patients in larger accidents. Moreover, it is easier to work resolutely on a patient who does not scream in pain while anaesthetized, in turn with a positive effect on the time spent on the scene and the quality in the field stabilization offered, as far as this can be of any help. We have exercised a liberation technique with the local fireworks, enabling a rather fast liberation of confined patients. The sad record in my on-scene times, 59 min, occurred in a nightly mission on a main street, 15 km away. This was one of the accidents after which I could not sleep, although I could have had at least an hour at the pillow that Sunday morning-
(23) Late one night, a couple of young men were on their way home from a visit to a discothek as their car suddenly gained affinity to one of the birchtrees which delineated the straigth road. Here, it remained in an incredible position, on the right side but with the roof up against the tree. It did not look as compatible with continued life for the insiders but to my great surprise, both were responsive, suffered great pain and in great fear of what might come. We shared their fear since it was not clear, how we should get them out of this wrack alive. At first, we supported the upper torso of the driver with a strap, releaving the passenger of his weigth. Now I asked the paramedics to require the helicopter since we, in case both patients were liberated alive, had better distribute them to two different hospitals; with a longer starting time at night, it was better to require the helicopter right away. Then I tried to enter through the window in the back but received an electric jolt. Having reminded the fireworkers to disconnect the car battery, I resumed the intrusion. I have often entered car wrecks but this was one of the most adventurous of such excursions. The intravenous accesses which I established on both patients had the purpose of giving way for pain-killers (amalgesia) and drowsymaking drugs (sedation), whereas the intravenous volume substitution is rarely important. So, if all other measures would be in vain, the two accident victims had already received some help.
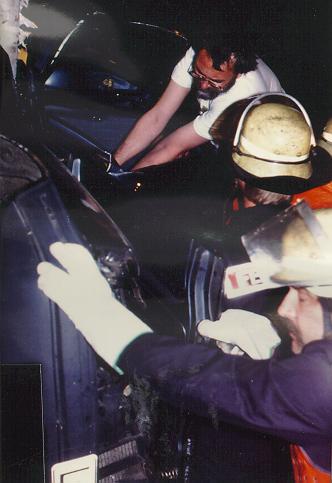
Fig 4: In this car wreck, which is standing on its side with the roof against (partly around) a birch tree, two young men are lying awake, confined, with serious pain and anxiety for their life (23).

Fig. 5: Anaesthesia is induced only after the car is taken down from the tree and the roof removed (if urgent, I had attempted it in the wreck before) (23).

Fig 6: Rescue of the two victims, now anaesthetized (23).
Fortunately, it came to more than that. As the car was about to be drawn down, I noticed from the inside that both men had a hand in the dangerous area. The procedure was interrupted and the hands liberated. In the meantime, the helicopter had landed and I went out to inform the colleague from Basel. We agreed that, once occasion would come, he should take care of the patient at the right who was presumably more injured. But as the car finally came down from the tree, the two men were still confined in it, until the roof was cut off. Simultaneously, we had access to the two men and this is the reason for me to claim this solemn case to be a comparison between my methods and the generally exerted ones. The driver now received etomidate, was intubated through the nose but, at first, not ventilated, i.e. he breathed spontaneously and we had hands free for the liberation. We have noticed that it is not only good for the spine but in general more easy to get confined patients out of a car-wreck when they are removed vertically along a scoop-stretcher, so this was what happended next. On this, the patient was transported to the vacuum-mattress (already prepared on the real stretcher) where the scoop-stretcher was then removed. Only when arriving in the ambulance, a ventilator was attached and the paramedics requested to attach the usual monitoring (for blood pressure, ECG and saturation). In the meantime, I went back to the other patient. Seing that the reverse order had been practised there. My help was not needed, so we slowly started the transport, driving towards Lörrach with our patient. Only 29 minutes later did the helicopter take off (in this case, time was not of importance). Both of the young men could be weaned from the ventilator after about one days therapy and recovered fast from their dangerous drive.
(24) In order to understand a bit more of this rescue technique, I shall utilize some photos I have from one of the rare missions to one of our two motorways. A car had left the road and was stopped by a tree after having rolled around. On the hind seat, a woman was seated, now with spinal injury and associated paresis – fortunately, she was left in the car until we arrived. While we attached a neck collar (always to be used by this injury, 20% have a second fracture at some distance from the one leading to the symptoms!), the firework demounted the roof (Fig. 7) as usual. Having finished creating the cabriolet, the patient was drawn up along the scoop-stretcher (Fig. 8) which slowly declined in response to her weigth. She was placed on the vacuum-mattress, which had been prepared just adjacent to the car. In the meantime, the helicopter had landed, with which she was flown to Basel. The chances of recovery are better with airtransport, even for smaller distances. We have used this method often before and after, but never with such impressive pictures. Previously, we had tried a so-called "extraction device", but its use is not so uncomplicated and it is incomparible with the vacuum-mattress.

Fig. 7 Removal of the roof from a car (24). Fig. 8. Vertical rescue over scoop-stretcher (24).
In the continental Europa, stabilization in spinal injury should generally follow this model. In North America and Great Britain, however, another invention is preferred, "the spine-board," which is a completely straigth plate (thus even worse than an operating table), to which the victim is attached with straps. It hurts very much to lie there, even without a fractured spine, but nothing doing: this is what the guidelines demand. Leading a symposium in Baltimore in May 1997, I tried in vain to make aware of the alternative which supports the spine when formed before the air is evacuated. Prehospital emergency medicine was a stimulating area in earlier earlier days when even the emergency departments of the hospitals had lost the lead. Strange that it has now come to a stagnation, not in spite of but as a consequence of the many persons who are involved in improving it further. Their efforts can only be compared to that of a missionaire: spread the dogma as far as possible without altering anything of its basis.

Fig 9 An X-ray of the spine with artifacts from a bad vacuum mattress.
The criticism can be continue towards radiologists, who are disturbed by certain shadows from the bag containing the polystyrol balls i the vacuum mattress - but I should admit that this is not equally bad for all of them. My remark that "radiologists prefer good pictures to good patients" was not well heard. Nevertheless, it remains a problem to avoid unnecessary manipulatioln before at least a surveying picture of the spine exists. I can imagine that future diagnostic principles (spiral-CT of seriolusly wounded in some 5 minutes, to be evaluated only when the patient has returned to the Emergency Department) can change the principle and also make a combination of the vacuum mattress with a non-pneumatic "antishock-principle" preferable. There is, of course, a risk associated with a foreseable devaluatory use of this method: "Tell me what came out of the spiral-CT, so that I can decide if it is necessary also to get out of bed ..."
(25) Once I really regretted to have entered a carwreck. A French car had been hit from the left (both doors demolished) and was now thrown into a pit (right doors up against the walls of the pit). The driver and two children, though injured, had emerged through the side windows, whereas the front seat passenger was to corpulent to permit that, in addition to suffering an asthmatic attack. I swung myself into the open window – and regretted it immediately. There was a heavy smell of gazoline and it had been a small comfort for the patient if I had been loyally burned together with her. Fortunately, the fireworkers came soon after and covered everything with foam before they violently opened the left front door. At this time, the patient’s asthma was under control with intravenous drugs and her liberation hence uneventful
(26) She was probably rather adipose as she entered the apartment, but somehow it was unnessecary for her to leave it through more than 10 years. Then she (forstuvede) her foot and a doctor came and prescribed an X-ray examination. A small ambulance came to get her but only now it was realized that the lady was too thick to leave the apartment trough the door. There was, however, a broad kitchenwindow and the fireworkers, always hoping for an unusual mission, gladly arrived with their special ladder with a mounted stretcher. Only now, I was also required to supervise the evacuation. I decided that the stretcher was heavy enough without my contribution and just provided a tranquilizer, not just for the coming flight but rather since the street was now filled up by curious on-lookers. I found the firemen a bit too satisfied with their mission and said: "Just stay where you are, we are just taking the patient to an x-ray examination and bring her back in a quarter of an hour". She never returned to that apartment.
(27) I clearly remember the accident by which I was most exhausted. I flew with the helicopter to a strange accident in the steep slopes of the Black Forest, so steep indeed that a tractor, in coming off the road, landed in the roof of a farm situated below. The farmer did not see anything funny in that, he was trapped between the tractor and pillars of the roof, and if he was liberated fastly, he would either fall backwards with the tractor or down into the house, with additional injuries resulting. He had enough already to justify an intubation immediately, but it was not absolutely necessary, he was still responsive and an intubation there on the roof would be associated with considerable risks for myself. I restricted myself to an infusion and an analgesic. Having done so, the man got weaker and needed my continued support. The firemen chose to attach a rope to the tractor, thus preventing it from falling, while a part of the roof was cautiously demounted. It took about half an hour to liberate him, and during this time I had to stay where I was, supporting him and avoid falling myself. When we had finally returned to firm soil, my whole body was shaking but in particular the hands from fatigue. I utilized the presence of a rescue ambulance in the further treatment, it was good to be able to close the door and her was ample space, quite contrary to the helicopter. Foremost, there were no wittnesses to observe my shaking hands while the patient was now intubated. We flew him to Basel and he survived the accident without any problems – never mind the rest. What I learned on that occasion was not to spend my forces on such an action when I thereby possibly disqualified myself from being able to help when my time – exclusively mine – then finally arrived.
(28) Then there was the mission where I got most wet. Twenty km from Lörrach, a worker had fallen down into a water reservoir which was almost empty. This accident gave him a serious fracture of the spine with associated paralysis. The problem was to get him out of this reservoir, the only access being a small opening in the ceiling, without destabilizing the fracture further by compression from the tilted stretcher. It is a wise rule to keep such considerations for one self, you can think of it while the basic therapy (analgesia through an i.v. line and stabilization with neckcollar, scoop stretcher and vacuum mattress) is carried out and afterwards demand some particular things as if every aspect of this mission was a matter of routine [Fig. 10]. Since I had arrived with the helicopter, I had already asked for their vacuummattress, which is narrower; now I demanded the shoulder-strap which is used to draw persons of in rescue missions. We had to utilize the scoop-strectcher below the vacuummattress, the normal stretcher being too broad for the opening. Two lines were tied to this while a third one was connected to the shoulder-strap.The eventual success of this action depended on that the policemen above the tank would make a stronger draught to the latter [Fig. 11]. In this case, precise instructions, without any haste for that, payed off. In spite of all improvisations, everything went well. The patient was flown to Basel where an operative stabilisation of fractured lumbar spines was carried out, eventually resulting in his ability to walk again.

Fig 10: Improvised rescue in the watertank (28).

Fig. 11: In this phase, it was
particularly
important that the patient was lifted up under the shoulders (28).
Next Chapters:
A dirty job
Dyspnoea
Problems are arising
Revised May 15, 2001