Died in accident (police statistic)
430
Mission protocol
239 100 %:
Died prehospitally without CPR
94 39 %
Died on site after CPR
43 18 %
Died in hospital after CPR on site
11 5 %
Died in hospital w/out prehosp.
CPR 91 38 %
100 %
Haemorrhagic shock
49
54 %
Responsive after accident
25
27 %
Table 1: Traffic accident fatalities in Lörrach County 1980-1996.
We examined the patients with a fatal accident according to a list made by the traffic police of Lörrach County during 17 years [Table 1]. The first reduction was necessitated through the absense of protocols in 191 cases, leaving 239 for further consideration. If only the patients are considered without prehospital cardiac arrest, then 54% of these were in a haemorrhagic shock and 27 % were not unconscious. For greater details, but therefore accepting a smaller number of cases, I studied the 60 fatalities from this list where I had been involved [Table 2].
60 fatalities registered (1982-96),
of them:
30
dead on site
3 seen only for secondary transfer
27
died after admission, of them:
13 awake after accident, of them:
2 thoracic bleeding *
7 intra-abdominal bleeding *
1 3° burns, 95%
2 postoperative complications §
1 delayed ARDS after thoracic trauma §
14 comatose after accident, of them
3 intra-abdominal bleeding *
1 old-age multitrauma (not intubated) *
2 head trauma with CPR on site *
4 isolated head trauma
2 other multitrauma
Table 2: Analysis of 60 traffic
accident fatalities of a the author. * Death within 4 hr after admission;
§ 3 patients intubated
> 48 hr after admission
In three cases, I saw the patients only for secondary
transfer and in another 30 cases, the patients were pronounced dead outside
the hospital, with or without a brief CPR. Among the remaining 27 patients,
abdominal haemorrhage was the cause of death in 10 patients and thoracic
bleeding in another two. Distinguishing between primary comatose and responsive
fatalities, roughly half of the latter died from abdominal bleeding.
In conclusion of this study, performed in an area of
advanced and aggressive prehospital emergency medicine, haemorrhage now
evolves as the predominant cause of death among primarily responsive accident
survivors. The next question was, if there was anything to do against it.
At this time it must be understood that if such a measure is found, such
a cause of death shall be considered preventable henceforth for the cases
where the method was not applied.
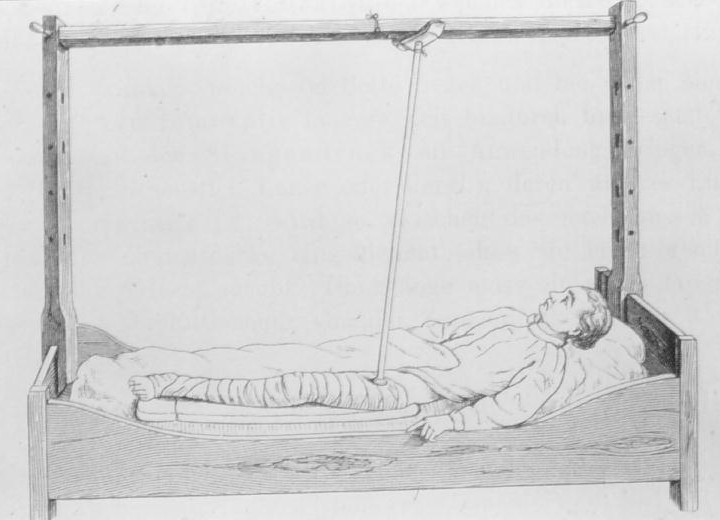
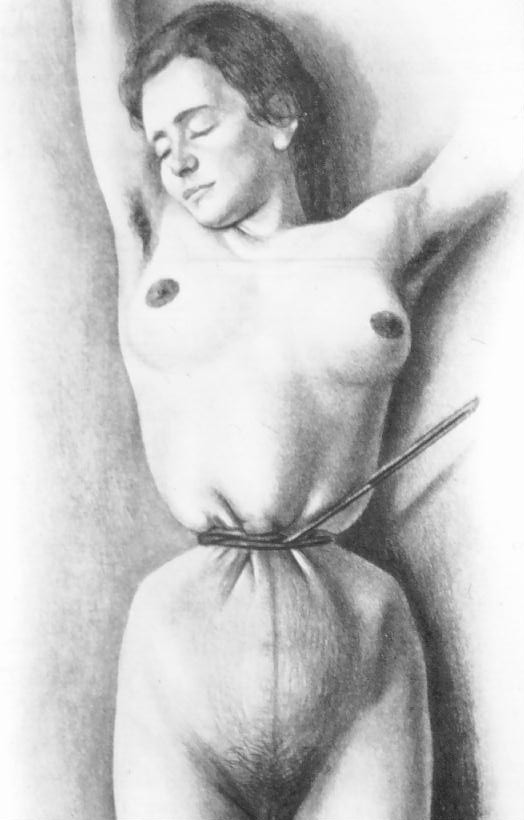
Fig. 1: Compression (patency protection
pending) Fig. 2: Momburg's compression
It is an old and often repeated observation, that it is
possible to halt external (visible) bleeding through compression. This
claim is certainly not subject to any controlled studies, such a study
would violate basic ethics. In the meantime widely forgotten, compression
has also been used against internal bleeding sources, both in the 19th
and the first part of the 20th century. Many principles and devices have
been constructed for this purpose, among them the compression the the lumbar
aorta in cases of postpartal atonic bleeding, described by J. Momburg (1870-1939).
From a logical point of view, these were the predecessors to the pneumatic
antishock-garment [PASG] described 1904 by Crile [2]. From the desire to
apply abdominal compression, we therefore instituted a non-pneumatic version
of Medical Antishock Garment [MAST] in our rendez-vous ambulance in 1996.
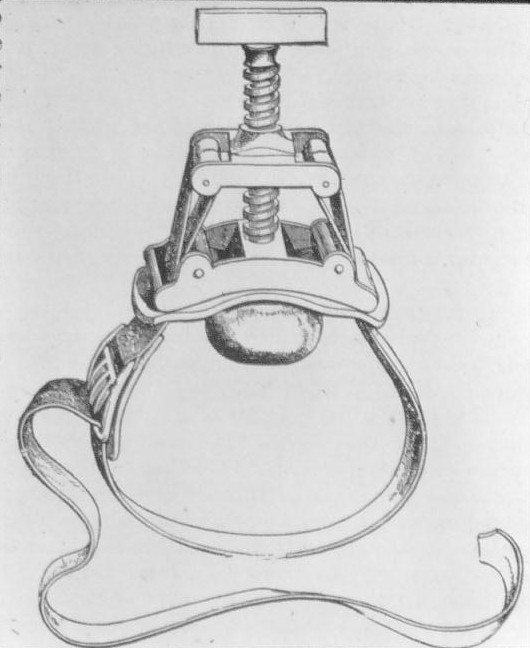
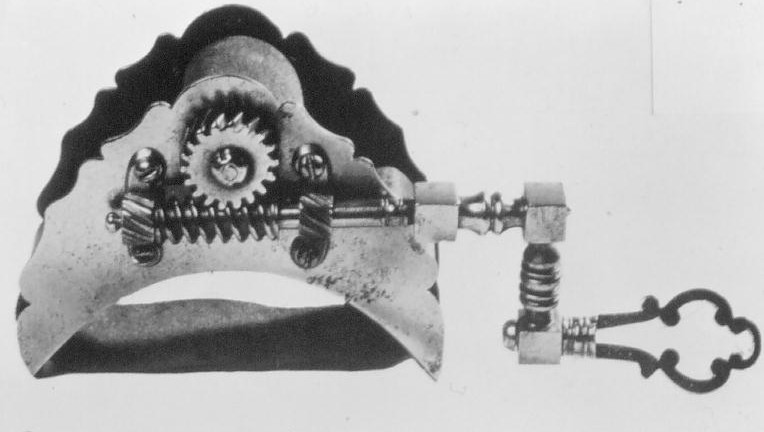
Fig.s 3 & 4: Some older devices for abdominal compression, by courtesy of Prof. Jörg Waninger (with Fig. 1)
For incidental reasons, our first uses of MAST did not concern traffic accidents. Among them, two patients with aortic bleeding and pre-final haemorrhagic shock received it, with restoration of their circulation (in one case even need for antihypertensive therapy by the short-acting betablocker esmolol) and subsequent transfer to successful operation in Basle [3]. A review identified four other case-reports with identical conclusion [4-7]. If compression can act upon this disease with an only secondary effect upon the shock, we believe it must also be useful for venous and organ bleeding.
This was not supported by another review of MAST/PASG [1]. However, it was soon clear that not the impact upon bleeding, but that upon shock was the issue studied, according to the name of these devices which includes the concept of Antishock. In particular, the two randomized studies [8,9] do include many patients with thoracic bleeding. In a previous review, McSwain [10] found thoracic trauma to be a counter-indication to PASG. From a logical point of view, it must be considered wrong not just a waste of timne to increase the blood pressure in e.g. thoracic bleeding if you are incapable of acting against blood loss simultaneously. Moreover, the exclusive American studies did not utilize physicians on site and hardly intubated the patients in advance of applying MAST, making this measure much more dangerous later on.
MAST is very painful in the presence of abdominal bleeding, and just for that reason, we soon set anaesthesia as a precondition, only permitting others to start compression of the legs while we were securing the airways. These patients generally do not anticipate the emergency and have a full stomach, thus increasing the risks of aspiration if intubation is carried out only after applying abdominal pressure. Unfortunately, anaesthesia and intubation also pose risks of adverse effects [11], a risk to be balanced with the expected advantage of halting bleeding.
At this point, it is necessary to stop and reconsider
the message delivered here. I am uncapable of delivering figures showing
that external abdominal compression (e.g., originating in MAST) may reduce
fatal abdominal bleeding. This issue has not been studied by anyone. The
use of logical arguments is not in favour nowadays where randomised controlled
trials [RCT] and evidence-based medicine [EBM] decides about
the opinions. In order to strengthen my arguments, but therefore losing
sympathy with the majority of physicians devoting themselves to this principle,
it turns necessary to fight back in making aware of some weaknesses in
EBM [Table 3]. Considering the first nihilistic effect of EBM, it seems
that MAST lost credit in American studies because it was used wrongly,
in wrong patients and under the wrong assumption. Rarely were these patients
intubated in advance, they often had counterindications for MAST and the
option was Antishock, not to stop bleeding. In consequence, MAST is losing
sympathy. Was it perhaps once used too often (and wrongly) and now too
seldom?
1st nihilistic effect of EBM:
If you use a method wrongly,
an RCT will probably show
that it does not improve therapy.
2nd nihilistic effect of EBM:
What cannot be studied by RCT is always
claimed negative and speculative.
3rd nihilistic effect of EBM:
Guidelines necessarily refer to old principles.
New principles are therefore always in contrast
to existing guidelines; in turn, they are not studied.
Table 3: Nihilistic effects of Evidence-Based Medicine [EBM] (EBM is a man-made construct, in which thevidence of a clinical issue is weigthed, giving preference to RCT and meta-analyses of the same).
Should you believe in the possibility also to minimize internal abdominal bleeding through compression, the exact limits to the therapy remains open to further study. It seems possible to minimize bleeding from pelvic fracture as well as that caused by spleen and liver rupture, obstetric bleeding and even aortic aneurysm. Other sources (e.g., gastric bleeding) must currently be considered purely speculative targets.

Fig. 5: CT of author with non-pneumatic MAST (invisible - visible is my belt, which I forgot to take off).
We have decided to utilize the non-pneumatic version of MAST. It was effective in meanwhile three cases of prefinal aortic aneurysm and poses other advantages, among them the capability to perform computed tomography by X-ray or even magnetic resonance (absense of metal parts). Another advantage, of importance for air-rescue, consists of the stabile compression independant of flight heigths and the absence of manometers to steal the doctors attention.
I wanted to create a new principle, combining this device with the vacuum mattress [VM], but then we noticed other problems with that device. And suddenly, the spine board [SB] entered our peaceful sphere.
With any fracture, also spinal ones, immobilisation must be considered to decrease nervous damage. If the uncomfortable strapped patients on the spine-board can be considered immobilized, is a question of its own, but that is what ATLS recommends. Due to the risk of tissue necrosis, its use is restricted to two hours, which certainly does not cover both the prehospital and diagnostic in-hospital phase until operation. Worse, the Cochrane register recommends controlled, placebo based studies, which I at least consider roughly unethical.

Fig. 6: Artifacts disturbing radiological examination
At least, it is true that the vacuum mattress may produce very disturbing artifacts, and that was the target of our first study [12]. From that, you can at least see that there is a big difference in this production of artifacts.
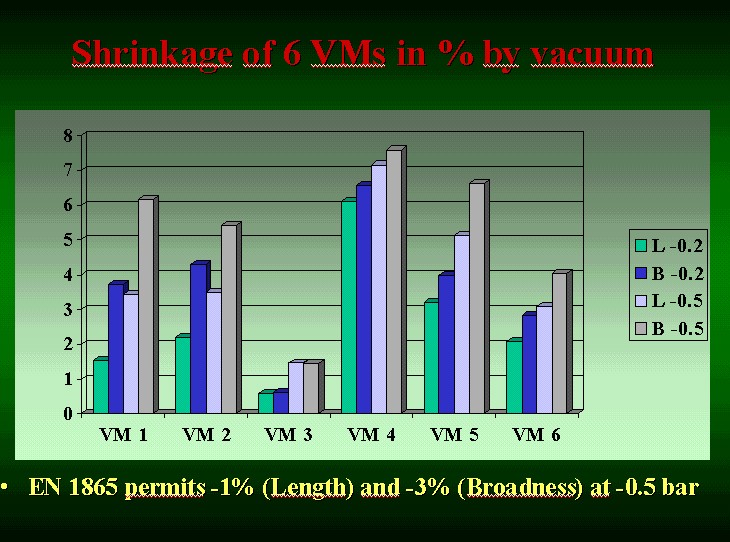
Fig. 7: Shrinkage of 6 different VMs, only tolerable in one. By courtesy of Dr. Winfried Reichert.
Much worse is another phenomenon, which we have only started to study. These data have not yet been published. You can see that only one of the mattrasses studied reaches the demand set by the European Norm. The others do more or less cause a compression upon the spine when air is evacuated.
It is therefore possible to improve the vacuum mattresses
themselves and, to my mind, this is the only suitable way of stabilizing
patients suspected of spinal injury. It is also required to improve the
European Norm, which is today acting against the use of this rescue device
in the diagnostic phase. I could not offer you much help against any use
of the spine board, which is protected by strong dogmatic forces, but you
can test its effects yourself in lying down on the floor at home 10 minutes
should suffice, if there is no carpet.
References:
1. Schou J, Ginz HF, Herion H-P, Huck D, Blum R,
Fehlmann R, Ummenhofer W. Abdominal haemorrhage a preventable cause
of death after field stabilization? Resuscitation 2000;43:185-93.
2. Crile GW. The resuscitation of the apparently
dead and a demonstration of the pneumatic rubber suit as a means of controlling
the blood pressure. Trans So Surg Gynecol Assoc 1904;16:361-70.
3. Schou J, Hauser E, Schreiner W. Use of
non-pneumatic antishock garments for ruptured abdominal aortic aneurysm.
Eur J Emerg Med 1997;4:169-71.
4. Burn N, Lewis DG, McKenzie A. The G-Suit:
Its use in emergency surgery for ruptured abdominal aortic aneurysm. Anaesthesia
1972;27:423-7.
5. Walsh K. Ruptured abdominal aortic aneurysms.
Amer Fam Phys 1981;24:26-9.
6. Gustavson RA, McDowell DE, Savrin RA.
The use of the MAST suit in ruptured abdominal aortic aneurysms. Am Surg
1983;49:454-9.
7. Dietze T, Uhlig HE, Kretschmer D, Hirt
R. Antishockhose: Lebensrettende Sofortmassnahme bei einem rupturierten
abdominellen Aortenaneurysma. Notfallmedizin 1989;15:457-60.
8. Mattox KL, Bickell W, Pepe PE, Burch J, Feliciano
D. Prospective MAST-study in 911 patients.. J Trauma 1989 29:1104-12.
9. Chang FC, Harrison PB, Beech RR, Helmer SD.
PASG: does it help in the management of traumatic shock? J Trauma 1995;39:453-6.
10 McSwain NE. Pneumatic anti-shock garments: state
of the art 1988 Ann Emerg Med 1988;17:506-25.
11. Schou J. Three techniques for prehospital emergency
anaesthesia. JEUR 1994;3:139-45.
12. Schou J, Kiermayer H, Ummenhofer W, Herion H-P. In
Search of the Most Suitable Technique for Truncal Spinal Immobilization
with Associated Radiography. Eur J Emerg Med 2001;8:89-92.
Preliminary version, July 9, 2002,
after lecture at TraumaCare, May
23-25, Stavanger, Norway.